
SEASONAL HEALTH | ENT
Spring allergies or a cold: how can you tell the difference?
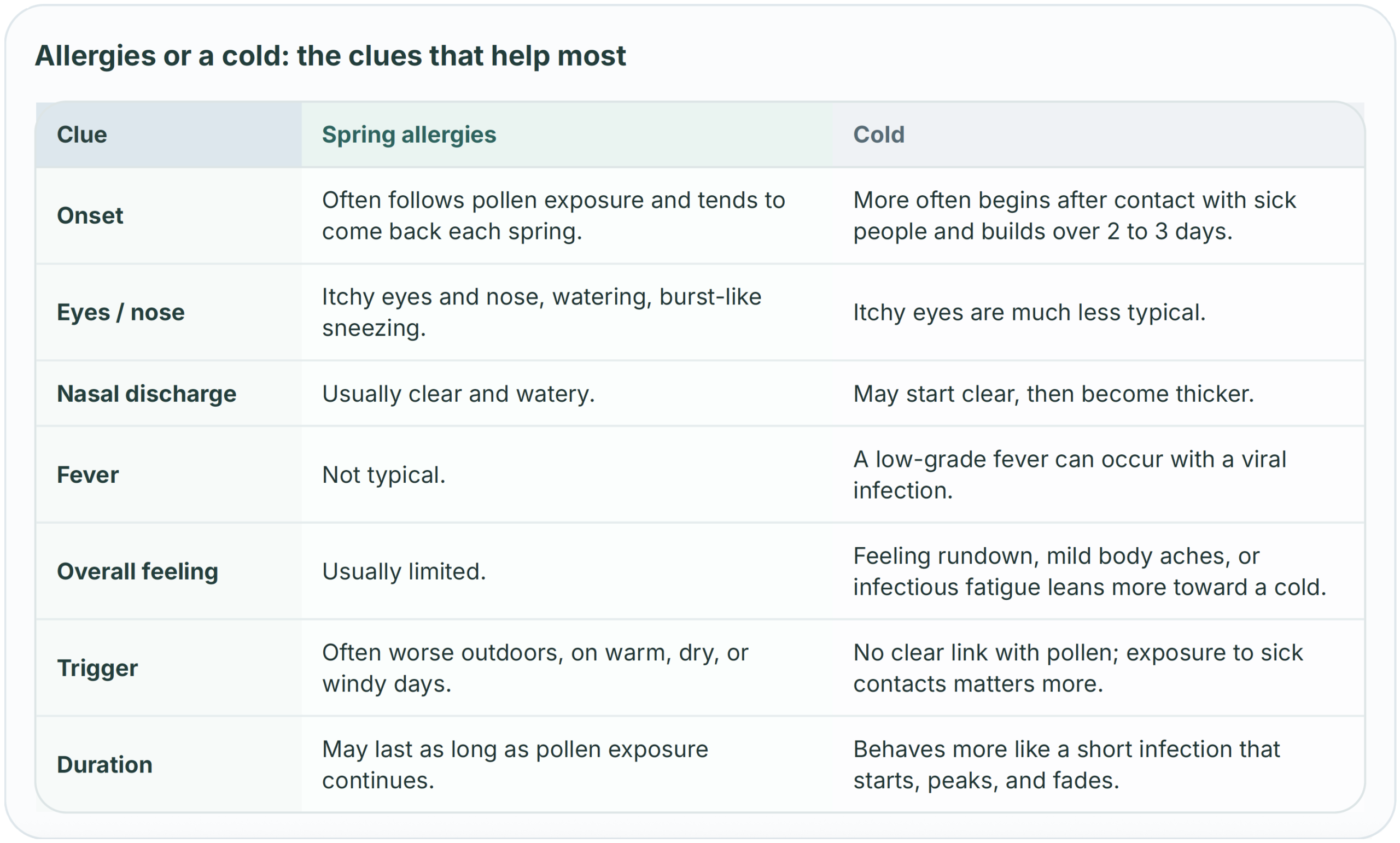
Stuffy nose, sneezing, a scratchy throat, itchy eyes… in spring, it is not always a cold. Here are the clues that help most, what may help at home, and when it makes sense to get assessed.
What points toward allergies
Itchy eyes and nose, burst-like sneezing, clear drainage, symptoms that come back each spring and often feel worse outdoors.
What points toward a cold
Sore throat, cough, recent contact with sick people, feeling more run down, and sometimes a low-grade fever.
When to get advice
If symptoms persist, affect sleep or work, or come with wheezing, shortness of breath, fever, or chest symptoms.
Start with context, not one symptom
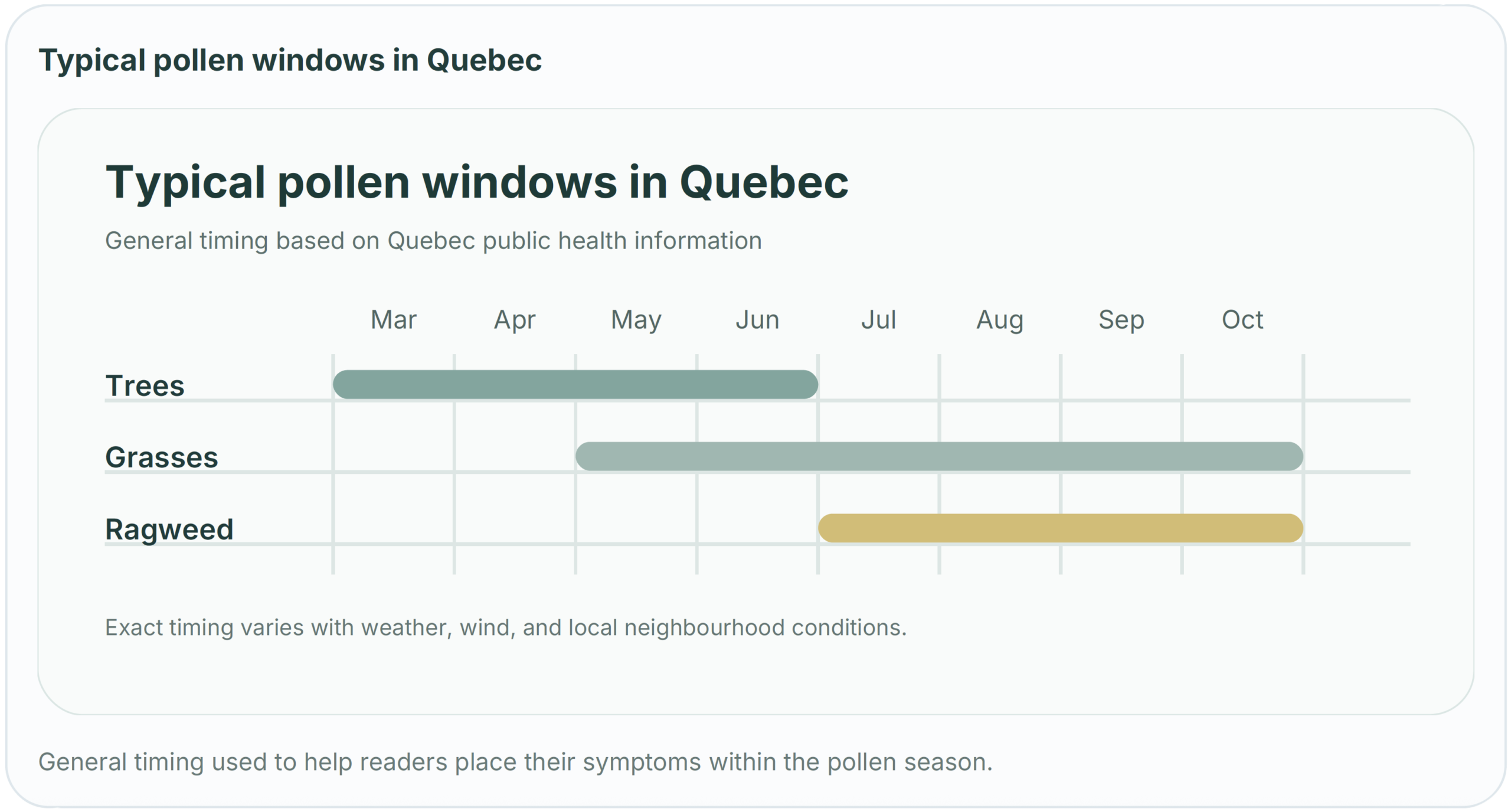
In Montreal, the first genuinely mild spring days often bring the same scene: windows open, park walks return, and suddenly there is a runny nose, nonstop sneezing, and a throat that feels irritated. Many people assume they are coming down with a cold. But in Quebec, seasonal allergic rhinitis affects about 1 in 5 people, and pollen season stretches longer than many realize: tree pollen is usually highest from March to June, grass pollen from May to October, and ragweed from July to October.[1] A 2024 JAMA review describes classic allergic rhinitis as a combination of congestion, runny nose, postnasal drainage, sneezing, and itching of the eyes, nose, or throat. By contrast, the CDC notes that the common cold is a viral upper respiratory infection: symptoms usually peak within 2 to 3 days, most colds last less than a week, and cough, sore throat, mild body aches, or a low-grade fever lean more toward a cold than seasonal allergies.[2][3]
The first useful clue is therefore timing — and the way symptoms repeat. If the same pattern comes back every spring, especially after a park walk, a windy day, or a warm dry morning, allergies become more likely. If symptoms started after contact with sick people, built gradually over 48 to 72 hours, and mainly make you feel generally unwell, a cold stays higher on the list.[1][3]
The clue that points most toward allergies: itching
When the eyes itch, water, or turn red, the nose itches, and sneezing comes in bursts, the needle moves more toward seasonal allergies. Nasal discharge is often clear and watery. Many patients also describe irritation in the throat or even the ears. Those details matter because they are much less typical of a simple cold.[1][2] Fever, on the other hand, is not part of the usual seasonal allergy picture. If you have body aches, a more obvious sick feeling, major fatigue, or a clearly painful sore throat, a cold or another respiratory infection deserves more weight.[3]
What leans more toward a cold
Cough, sore throat, and the sense that you have caught a bug point more toward a cold, especially if symptoms ramp up over a few days. That does not mean allergies never irritate the throat or cause a mild cough; the JAMA review also notes the role of postnasal drainage and the overlap with asthma. But if there is no eye itching, no clear link with outdoor exposure, and fever is part of the picture, the allergy label becomes less convincing.[2][3] Another practical test is to ask when and where you are worse. Allergies often have an “outdoors + repeat pattern” profile. Viruses spread mainly through close contact with sick people. If several people in the home start sniffling two days after one child brought a virus back from school, a cold quickly moves up the list.[3]
What may help now
If the pattern looks allergic, simple exposure-reduction habits often help more than people expect. Quebec recommendations include limiting outdoor exposure when pollen levels are higher — especially from 7 a.m. to 1 p.m., on warm or dry days, and on windy days — keeping windows closed when possible, wearing sunglasses outside, and changing clothes when you get home.[1] When symptoms keep returning or begin to affect sleep, work, or concentration, a pharmacist or clinician can help choose an over-the-counter option that fits. The 2024 JAMA review notes that mild intermittent allergic rhinitis may respond to a second-generation antihistamine or an intranasal antihistamine, whereas more persistent or more severe symptoms are often initially managed with an intranasal corticosteroid. A 2024 JAMA patient page also points out that nasal steroid sprays are not always immediate: some improvement may begin within 12 hours, but full benefit can take several days of regular use.[2][4] More recent evidence points in the same direction. A 2024 systematic review and meta-analysis in the Journal of Allergy and Clinical Immunology found that most intranasal medications improve nasal symptoms, eye symptoms, and quality of life. The updated ARIA-EAACI guidance published in 2025 and 2026 adds an important nuance: the best choice depends on symptom pattern, severity, patient preferences, and cost. In other words, there is no single best option for everyone.[5][6][7]
When to get checked
It is reasonable to seek care if symptoms persist, affect quality of life, or are not relieved by over-the-counter treatment. Earlier assessment also makes sense if there is wheezing, shortness of breath, repeated sinus infections, or worsening asthma.[1][2] If there is fever, significant body aches, heavy cough, chest symptoms, or exhaustion that feels more infectious than allergic, it is wise to think beyond seasonal allergies. The CDC also reminds patients that COVID-19, influenza, and RSV can cause cold-like symptoms but may carry a higher risk of complications in some people.[3] In spring, the best habit is not to label every stuffy nose as just a cold. The pattern matters more: repeated seasonal symptoms, outdoor triggers, itching, and the absence of fever are often the clues that point toward allergies. When the picture is unclear, a clinical assessment can save time and help you get more appropriate relief.
When to seek care sooner
- If symptoms persist and interfere with quality of life.
- If over-the-counter treatment is not helping enough or is poorly tolerated.
- If there is wheezing, shortness of breath, repeated sinus infections, or worsening asthma.
- If fever, major body aches, heavy cough, or chest symptoms make an infection more likely.
Need help sorting it out?
For recurring spring symptoms, lingering congestion, or questions about the best next step for relief, the CYMED team can help distinguish allergic rhinitis, respiratory infection, and other common causes of nasal symptoms.
This article is provided for general information only and does not replace a medical assessment. Please do not send personal health information through blog-related forms or comments. A patient-physician relationship is established only when a CYMED clinician has accepted your care.
References
- Government of Quebec. Rhinite saisonnière (rhume des foins). Updated June 13, 2023. quebec.ca.
- Bernstein JA, Bernstein JS, Makol R, Ward S. Allergic Rhinitis: A Review. JAMA. 2024;331(10):866-877. doi:10.1001/jama.2024.0530.
- Centers for Disease Control and Prevention. About Common Cold. Updated February 19, 2026. cdc.gov.
- Vordenberg SE. Nonprescription Medications for Adults With Allergic Rhinitis. JAMA. 2024;331(3):268. doi:10.1001/jama.2023.20171.
- Sousa-Pinto B, Vieira RJ, Brozek J, et al. Intranasal antihistamines and corticosteroids in allergic rhinitis: a systematic review and metaanalysis. J Allergy Clin Immunol. 2024;154(2):340-354. doi:10.1016/j.jaci.2024.04.016.
- Sousa-Pinto B, Bousquet J, Vieira RJ, et al. Allergic Rhinitis and Its Impact on Asthma (ARIA)-EAACI Guidelines-2024-2025 Revision: Part I-Guidelines on Intranasal Treatments. Allergy. 2025;81(4):954-976. doi:10.1111/all.70131.
- Vieira RJ, Sousa-Pinto B, Bousquet J, et al. Allergic Rhinitis and Its Impact on Asthma (ARIA)-EAACI Guidelines-2024-2025 Revision: Part II-Guidelines on Oral and Ocular Treatments. Allergy. 2026. doi:10.1111/all.70305.